|
|
 |
| |
|
|
 |
Introduction |
|
Loss of thumb or digits after accident often results in cosmetic and functional problems to the patients. In congenital hand deformity, patients are not able to live a normal life because they loss some very important functions accomplished by normal hands.
After the first toe-to-hand transfer done in monkey in 1966 and the first one in clinical application by Cobbett in 1975, a series of refinement has been introduced to reduce donor site and recipient site morbidity. It is right now presents as a fine technique and a good choice in patients who want to have better hand function after trauma or in congenital hand deformities. This technique is widely used now and keeping refined for better functional and cosmetic results. |
| |
|
|
Indications toe-to-hand transfer |
|
The indications for toe transfer in hand trauma include (1) thumb amputation, (2) finger amputation distal to the sublimis insertion, (3) metacarpal hand reconstruction, and (4) pulp loss or insensibility. |
| |
|
|
Reconstruction Options |
| - |
Thumb reconstruction |
| |
In thumb reconstruction, the donor site could be the great toe or the second toe. For better aesthetic results, trimmed or wrap-around great toe may be used. The decision depends on the function and aesthetic requirement of the patients and the preference of the surgeon. Generally, great toe transfer presents better in thumb reconstruction both functionally and aesthetically. The second toe has smaller contact surface for opposition and a tendency to claw. However, the donor site function and aesthetic result is worse in great toe transfer. Generally, second toe is better done in patients with an almost thumb-size second toe or in patients who demand minimal foot deformity or less functional requirement in the reconstructed thumb. (For example, in the non-dominant hand or in old age patients) The great toe is the best choice in patients who have a severely injured hand and require optimal thumb function. |
| - |
Finger reconstruction |
| |
In finger reconstruction, several questions should be considered: (1) how many digits to be reconstructed (2) where these digits to be positioned (3) which technique to be used. To aim on better functional result, there are several principles: (1) to allow useful tripod (chuck) pinch (2) enhance lateral stability (3) provide stronger hook grip (4) provide wider span for grasping large objects. Besides, the decision should be made individually. For labors who require powerful grasp, reconstruction of the ulnar digits is the best. For patients requiring fine hand movement, reconstruction of the radial digits is better.
The second, third and fourth toes could be used in digit reconstruction alone or in combination. In reconstruction of two adjacent digits amputated proximal to the web space, combined second and third toe transfer is indicated. Amputations distal to the web space are best reconstructed with two isolated second toe. Sometimes, the third toe could be used when the second toe has been transferred or injured, or when the third toe provides better size match.
|
| - |
Distal digit reconstruction |
| |
The glabrous skin of the digital pulp plays an important role in firm grip, pinch, and object handling and its precise sensation. In addition, the nail provides stability and cosmesis to the finger. Based on the reconstruction concept of ˇ§replace like tissue to like tissueˇ¨, the foot is good donor site in reconstruction of pulp and nail. |
| |
|
|
Refinement procedure |
| |
Although toe transfer is now widely used for the reconstruction of thumb and finger function and the function of the digit could be achieved well, the appearance of the reconstructed hand is also important for patientˇ¦s acceptance and the willing to use the reconstructed hand in daily life. The great toe is stouter and wider than the thumb. To trim the great toe during harvesting could provide better cosmesis of the great toe to the thumb. Wrap-around technique also provides better aesthetic result of the transferred toe.
In the donor site, well preservation of the metatarsopharyngeal joint of the great toe allows better functional preservation. Also, with carefully design of the wedge shape soft tissue flap, the donor site of the second or third toe transfer could also achieve a good-looking. |
|
Case presentation |
| - |
Case 1: |
| |
A 6-year-old male patient with crush amputation of right second, third, and fourth finger. |
| |
 |
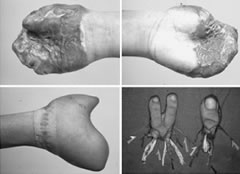
Fig. 1. (Above, left) Crush amputation of the right second, third, and fourth fingers. The amputation stumps were covered with a pedicle groin flap. (Above, right) Two years after simultaneous transfer of both second toes to the right index and middle fingers. (Below, left) Good prehensile function achieved. (Below, right) Two-year postoperative radiograph showing solid bony union and open physis of the middle phalanges of the transferred digits. |
|
| - |
Case 2: |
| |
A 7-year-old boy suffered from flam burn injury and presented to us with bilateral metacarpal hand. Release contracture and covered with pedicle groin flap were done, followed with trimmed great toe transfer to the thumb and combined third and fourth toe transfer. Release contracture and pedicle groin flap coverage were done in the non dominant hand and second toe transfer to the thumb and third toe for digit reconstruction were done. Pulp to pulp pinch in the non-dominant hand and tripod pinch of the dominant hand could be achieved. He could attend school without limitation. |
| |
|
| |
|
|
Relative articles |
|
| 1. |
Wei, F.C., et al.: Reconstruction of a hand amputated at metacarpophalangeal level using combined second and third toes from each foot. Journal of Hand Surgery. Vol. 11A, No. 3, P. 340-344, May, 1986. |
| 2. |
Wei, F.C., Chen H.C., Chuang C.C., Noordhoff M.S.: Simultaneous multiple toe transfers in hand. Plastic and Reconstructive Surgery.81(3):366-374, 1988. |
| 3. |
Wei, F.C., Chen H.C., Chuang C.C., Noordhoff M.S.: Reconstruction of the thumb with trimmed-toe-transfer. Plast Reconstr Surg. 82(3):506-513, 1988.. |
| 4. |
Wei FC, Colony LH, Chen HC, Chuang CC, Noordhoff MS: Combined second and third toe transfer. Plast Reconstr Surg. 84(4):651-662, October, 1989. |
| 5. |
Wei, F.C., Chen, H.C., Chuang, C.C., Chen, S., Noordhoff, M.S.: Second toe wrap-around flap. Plastic Reconstructive Surgery. 88:P837-843, 1991. |
| 6. |
Chen, H.C., Tang, Y.B., Wei, F.C., Noordhoff, M.S.: Finger reconstruction with triple toe transfer from the same foot for a patient with a special job and previous foot trauma. Annals of Plastic Surgery. Vol. 27, P. 272-277, 1991. |
| 7. |
Chen, S., Wei, F.C., Noordhoff, M.S.: Free vascularized joint transfer in acute complex hand injury. Journal of Trauma. 33(6):924-930, 1992. |
| 8. |
Wei, F.C., Seah, C.S., Chen, H.C., Chuang, C.C.: Functional and aesthetic reconstruction of a multilated hand using multiple toe transfers and iliac osteocutaneous flap: A case report. Journal of Microsurgery. 14:388-390, 1993. |
| 9. |
Strauch, R., Wei, F.C., Chen, H.T.: Composite finger metacarpophalangeal joint reconstruction in combined second and third toe-to-hand free tissue transfer. Journal of Hand Surgery. 18A(6):972, Nov. 1993. |
| 10. |
Wei, F.C., Chen, H.C., Chuang, C.C., Chen, H.T.: Microsurgical thumb reconstruction with toe transfer: Selection of various techniques. Plastic and Reconstructive Surgery. 93:2, P. 345-351, 1994. |
| 11. |
Wei, F.C., Strauch, R.J., Chen, H.C., Chuang, C.C.: Reconstruction of four damaged or destroyed ipsilateral fingers with free toe-to-hand transfer. Plastic and Reconstructive Surgery. 93:608-614, 1994. |
| 12. |
Graf, V.P., Wei, F.C., Groner, R., Biemer, E.: Second toe transplantation for partial amputation of digits - indication, planning, operative technique. Handchir, Mikrochir, Plast. Chir. 26:262-267, 1994. |
| 13. |
Wei, F.C., Yim, K.K.: Pulp plasty after toe to hand transplantation. Plast. Reconstr. Surg. 96:661-666, 1995. |
| 14. |
Wei, F.C., Yim, K.K.: Single third toe transplantation in hand reconstruction. Journal of Hand Surgery. 20A:388-394, 1995. |
| 15. |
Yim, K.K., Wei, F.C.: Intraosseous wiring in toe-to-hand transplantation. Annals of Plastic Surgery. 35:1, P. 66-69, July, 1995. |
| 16. |
Wei, F.C., Chen, H.C., Chuang, C.C., Jeng, S.F., Lin, C.H.: Aesthetic refinement in toe to hand transfer. Plast. Reconstr. Surg. 98:485-490, 1996. |
| 17. |
Wei, F.C., El-Gammal, T.A.: Toe-to-hand transfer: Current concepts, Techniques and research. Clinics in Plastic Surgery. 23:103-106, 1996. |
| 18. |
El-Gammal, T.A., Wei, F.C.: Combined second and third toe transfer: current practice. Asian-Pacific. Hand Surgery. 1:11-16, 1996. |
| 19. |
Ma, H.S., El-Gammal, T.A., Wei, F.C.: Current concepts of toe-to-hand transfer Surgery and Rehabilitation. Journal of Hand Therapy. 9:41-46, 1996. |
| 20. |
Wei, F.C., El-Gammal, T.A., Chen, H.C., Chuang, C.C., Chiang, Y.C., Chen, H.T.: Toe-to-hand transfer for traumatic digital amputation in children and adolescents. Plast. Reconstr. Surg. 100(3):P605-609, September, 1997 |
| 21. |
Wei F.C.: Tissue Preservation in Hand Injury: The First Step to Toe-to-Hand Transplantation. Editorial Plast Reconstr Surg 102(7):2497-2501, December 1998 |
| 22. |
Chen H.C., Tang Y.B., Chen S.H.T., Wei F.C.: Improving the result of vascularized joint transfer in hand joints: two-stage reconstruction with two periods of rehabilitation. Techniques in Hand and Upper Extremity Surgery 2(4):262-268, 1998. |
| 23. |
Chu N.S., Wei F.C.: The time course of recovery in somatosensory evoked potentials and sympathetic skin response after toe-to-finger transplantation. Recent Advances in Human Neurophysiology P163-168, 199 |
| 24. |
Tan B.K., Wei F.C., Chang K.J., Lutz S.B., Chen S.H.T.: Combined third and fourth toe transplantation. Hand Clinics 15(4):589-596, Nov. 1999 |
|
| |
| |
|
|
|
|
|
 |