Laparoscopic TAH-BSO Part I
|
Revolutionary advancements in endoscopy have dramatically changed the practice of gynecology. With the introduction of the newest generation of endoscopic instruments, we have become more proficient in laparoscopically assisted hysterectomies with bilateral salpingo-oophorectomies.
There is still controversy as to whether traditional vaginal hysterectomy is the better procedure compared with its laparoscopic counterpart. Our experience with laparoscopic hysterectomy demonstrated that the laparoscopic approach is superior in most patients with myomas, previous cesarean sections, undiagnosed endometriosis, chronic pelvic inflammatory disease and unexpected intestinal pathology.
The greatest advantage of a laparoscopic hysterectomy is the significant reduction in postoperative pain, discomfort and the shorter recovery period. Compared to traditional open surgical procedures, laparoscopic hysterectomy has reduced the hospital stay and cost by 50%. The patient can return to work after 3 weeks versus 6 weeks. For these reasons, it is anticipated that laparoscopic hysterectomy will become the standard rather than the exception within 5 years.
| INSTRUMENTS |
Note: The telescope used in these cases is a Storz straightforward telescope 0 with parallel eyepiece and 5mm instrument channel. A Storz Video system is used. All patients are given Toradol (Roche Pharmaceuticals) 30mg IM and Cefizox (Fujisawa USA) 2 Gm IV during the induction phase.
| THE PROCEDURE |
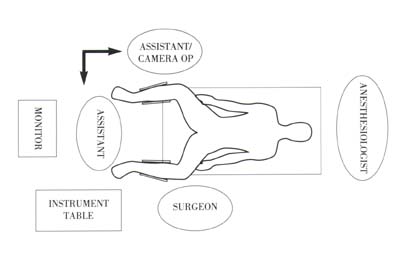
Operating Room Setup
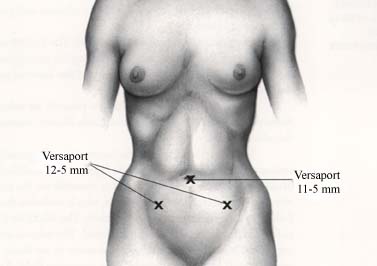
Trocar Placement
The Technique
The patient is placed in lithotomy position with Allen universal stirrups. A Kronner Manipujector is inserted. The abdomen and perineum are prepped in the usual manner.
The pneumoperitoneum is created. The trocars are inserted. The intraabdominal cavity is visualized. Using the uterine manipulator, the uterus and adnexa are moved, and all aspects of the internal genitalia are exposed and examined.
If intraabdominal adhesions are present, an enterolysis will be performed using the ENDO SHEARS* and ENDO DISSECT* instruments connected to the electrocautery.
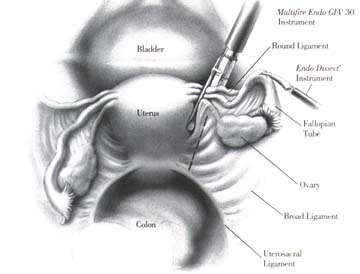
The ovary is grasped at its ligament and elevated with an ENDO DISSECT* instrument. The infundibulopelvic ligament is identified and spread. A Multifire ENDO GIA* 30 instrument is inserted via the ipsilateral 12mm trocar site and closed on the triple pedicle, which includes the round ligament, the fallopian tube and the ovarian ligament. The Multifire ENDO GIA* 30 stapler is fired and the triple pedicle transected. The tubo-ovarian complex will be separated from the uterus. If this maneuver is not done, the tubo-ovarian complex will constantly drop into the operating field. Another application of the Multifire ENDO GIA* 30 instrument will be needed to continue this dissection on the parametria.
The same procedure is repeated on the other side.
![]()