| Laparoscopic TAH-BSO - Part II
|
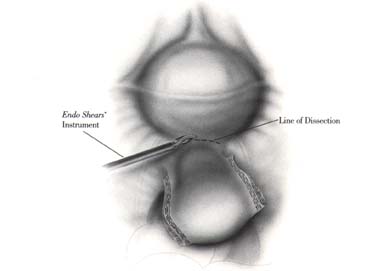
The operative site is brought into telescopic view by moving the Kronner Manipujector. The anterolateral aspect of the uterovesical junction is placed under tension. Using the ENDO SHEARS* instrument connected to an electrocautery source, the peritoneal bladder flap is developed in traditional fashion.
The dissection is started laterally and continued anteriorly around the cervix. The bladder flap is gently peeled away with the ENDO SHEARS* instrument. The hemostasis is controlled with electrocautery. The posterior sheath of the broad ligament is dissected down to the uterosacral ligament. The uterosacral ligaments are transected using an ENDO SHEARS* instrument.
The uterine vessels (artery and vein) are identified. At this level, they usually run parallel to the uterus. The ureter will also be lateral to the vessels and also parallel to the uterus. Stay as close as possible to the uterus while clipping, almost clipping the vessels into the cervix.

The assistant places a curved sponge stick into the posterior vagina.
A posterior colpotomy is made with the ENDO SHEARS* instrument. This vaginal incision is not made by cutting but merely by using the electrocautery power with the ENDO SHEARS* instrument to transect. It is performed slowly so that the pneumoperitoneum will not be rapidly lost (CO2 leak).
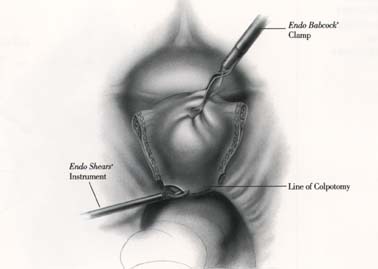
The vaginal will be packed and sealed with wet Kerlix gauze. The pneumoperitoneum is recreated. The colpotomy is completed anteriorly and laterally. The colpotomy is extended around the base of the cervix on the vagina until the uterus is detached from the vagina.

If a bilateral oophorectomy is to be performed, a Multifire ENDO GIA 30 instrument is inserted and used to staple and transect the infundibulopelvic ligament. The tubo-ovarian complex is then freed on each side.
The vaginal pack is removed. A large Kocher clamp is passed transvaginally into the intraabdominal cavity under direct vision. The uterus and both tubo-ovarian complexes are removed via the colpotomy.
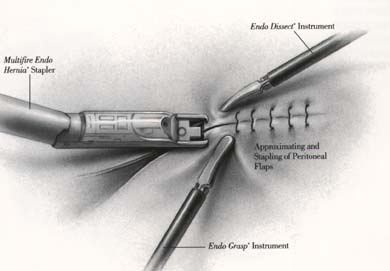
The colpotomy is then closed transvaginally with interrupted size 2-0 Polysorb absorbable sutures. The pneumoperitoneum is again created. The peritoneal edges are approximated with an ENDO DISSECT* instrument and with the extended grasper passed via the working channel of the telescope. A Multifire ENDO HERNIA* stapler is inserted via a lateral VERSAPORT* 12mm trocar and peritoneum is closed with Multifire Endo Hernia staples.
The abdomen is irrigated with Ringer’s lactate solution; desufflated and all the cannulas are removed. The 12mm insertion sites should be closed in a two-layer fashion.
References: