|
Laparoscopic Inguino-Femoral Hernia Repair
|
|
To date, the laparoscopic repair of inguino-femoral hernias has had a tumultuous beginning in the surgical arena. Laparoscopic repairs have had to compete with the current gold standard for anterior or conventional inguinal hernia repairs, the Liechtenstein repair. Initially, some of these laparoscopic repairs, such as the "plug and patch" (PAP) and "on lay technique" (IPOM ), failed to demonstrate good results and were abandoned. In 1996 and 1997, only two laparoscopic repairs have proven to be viable with early results comparable or superior to the Liechtenstein repair. These repairs are the Extraperitoneal Laparoscopic Repair (EXTRA) and the Trans-Abdominal Preperitoneal Repair (TAPP).
It should be noted, the most ardent critique of the TAPP procedure is that it is an intra-abdominal procedure with significant potential morbidity. For this reason, the TEP procedure which avoids intra-abdominal access was developed. In our studies, the morbidity rate of both these laparoscopic repairs was minimal and/or similar to other open repairs with comparable early recurrence rates. The most persuasive argument for using this procedure is the same argument favoring all laparoscopic procedures: the postoperative benefits to the patients, i.e., less postoperative pain, decreased disability and small incisions. However, it continues to be a new procedure with limited long term follow-up and analysis.
During the early nineties, our surgical team developed an original TAPP repair. This original technique was modified on several occasions. Later, the TEP technique was introduced for patients who had previously undergone major lower abdominal surgery. As of August 1, 1999, 1700 repairs were performed. Our technique and results are herein reported.
| INDICATIONS |
|
All patients cleared for general anesthesia were candidates for this repair. Our youngest patient was fifteen years old and our oldest 87 years old. Previous intraabdominal surgical procedures were not a contraindication. The surgeon decides on a per case basis if an extensive, lengthy enterolysis is in the best interest of the patient or if a TEP technique should be used. It has been reported that the major indications of this technique are recurrent inguinal hernias and bilateral inguinal hernias. We recommended that all inguino-femoral hernias including single, unilateral defects be repaired via laparoscopy.
| A TECHNICAL CONSIDERATION: UNDERSTANDING THE ANATOMY |
|
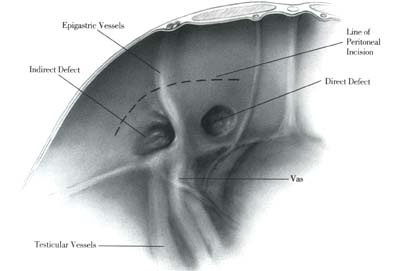
The anatomy of the inguino-femoral region viewed via a telescope placed in intra-abdominal position differs radically from the anatomy observed via an open or anterior approach. The laparoscopic surgeon needs to become familiar with the anatomical structure of this region. As all anatomical landmarks are covered with peritoneum, in the TAPP technique the peritoneum has to be first incised and a lower flap developed in order to expose the region adequately. In the TEP repair, the anatomical landmarks need to be meticulously exposed with blunt dissection.
Our guidelines for the performance of a safe and secure laparoscopic inguinal hernia repair, mandate the following structures should be clearly and unequivocally identified:
- Cooper's Ligament
- The Epigastric Vessels
- The Spermatic Cord or the Round Ligament
- The Femoral Canal and the Iliac Vessels
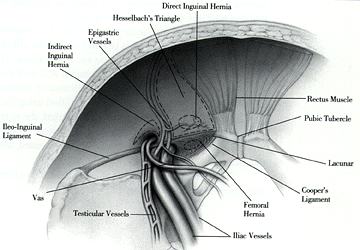
- In addition, the laparoscopic anatomical distinction between direct, indirect inguinal and femoral hernias should be well understood. Before a surgeon attempts to perform a laparoscopic inguinal or femoral hernia repair, he should memorize and be very familiar with the following diagrams.
Anatomy: Inguinal Region with Peritoneal Coverage
Anatomy: Inguinal Region without Peritoneal Coverage
Click on the following buttons to access each techniques
| The TAPP Repair | ||
| The TEP Repair |
| TECHNICAL NOTES |
|
- - Incarcerated Inguinal-Femoral Hernia: TAPP Repair,
- - Inguino-Femoral Hernia / Patients with previous major lower abdominal surgery: TEP Repair,
- - Massive Inguinal Hernias with scrotal extension: TEP Repair or Anterior Repair,
- - Bilateral Inguinal Hernias: TAPP or TEP Repair.