|
Laparoscopic Inguino-Femoral Hernia Repair |
|
||||||||||
| To view the original TAPP technique |
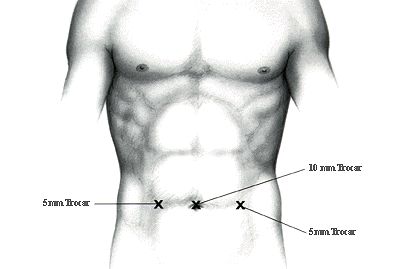
This modification was introduced in late 1995, early 1996. Although the actual technique is identical to the Standard TAPP technique described previously, the introduction of a new stapling device, the USSC 5 mm PROTACK* Instrument, has enabled us to perform this technique, using two 5 mm trocars and a 10 mm trocar or three 5 mm trocars. This variation eliminates the closure of the facial defect created by the 12 mm trocar (used to insert the 12 mm Multifire Endo Hernia* Stapler).
| Hardware Required |
|
- 1) Storz Zero Degree 10 mm Telescope,
- 2) Storz Camera (three chips or single chip),
- 3) Storz High Insufflator,
- 4) CO2 Tank,
- 5) High Resolution Sony Monitor 21 inches,
- 6) Optional Printer - Storz
| Anesthesia |
|
General Endotracheal Anesthesia is used. Each patient is injected in the Pre-induction phase with 60mg IM Toradol (Roches Pharmaceuticals) and with 2grs. of Cefizox IV (Fujisawa Laboratories)
| operating room set-up |
|
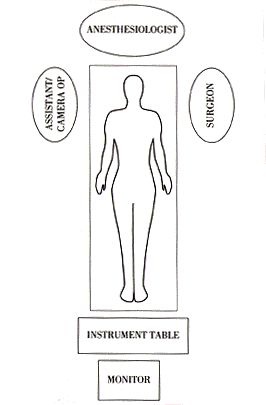
The patient is in supine position, arms tucked at the side. The surgeon stands at the head of the table opposite the hernia. No dedicated surgical assistant is used for these procedures. A scrub nurse/camera holder will sit at the head of the operating table across from the surgeon.
| Instruments |
|
- 1 Verres Needle or SURGINEEDLE*
- 2 USSC VERSAPORT* trocars -5 mm
- 1 USSC VERSAPORT* trocar 5- 11mm
- 1 USSC ENDO SHEARS* Instrument with cautery connection
- 1 USSC ENDO DISSECT* Instrument
- 1 reusable Storz 5 mm dolphin nose grasper
- 1 6" x 6" USSC SURGIPRO* Mesh (Open weave)
- 1 disposable USSC PROTACK* (30 tacks)
Note: In some cases, we have used three 5 mm trocars with a 5 mm zero degree telescope. However, the introduction of the SurgiPro* Mesh (Open Weave) is time-consuming and difficult. It has to be introduced without the trocar and pushed directly with an ENDO DISSECT* instrument into the intra-abdominal cavity.
| The Technique |
|
A pneumoperitoneum is created using a Verres Needle and an intra-abdominal pressure of 15 mm Hg is maintained. The 10 mm trocar in infra-umbilical position is inserted. The telescope is then inserted and the intraabdominal cavity explored. Two 5 mm trocars are inserted lateral to each Rectus Muscle, at the same level as the umbilical trocar.
STEP 1: Creating the Peritoneal Flap
The repair is initiated. The laparoscope is pointed toward the afflicted inguinal canal. The peritoneal defect or hernia is identified. The other inguinal canal is inspected. If an asymptomatic hernia sac is found on the other side, our protocol mandates its repair, even though at this time we are unsure of its exact clinical significance. The Lateral Umbilical Ligament is located as well as the Inferior Epigastric Artery and Vein. A peritoneal incision is made using the EndoShear* Instrument connected to an electrocautery source. The incision is extended from the lateral aspect of the inguinal region to the Lateral Umbilical Ligament. For obese patients, this ligament may have to be transected in order to obtain additional exposure. The operator should be meticulous in making this incision as high as possible to maximize the exposure of the region.
STEP 2: Exposing the Inguinal Structures
Using the Endodissect* Instrument bluntly, Cooper's Ligament is exposed as well as the Inferior Epigastric Vessels and the Spermatic Cord. It is essential to expose the uncovered abdominal wall meticulously (without peritoneum) and remove all fatty layers.
STEP 3: Dissecting the Hernia Sac
The indirect inguinal hernia sac should be dissected carefully from the Spermatic Cord. Particular care should be taken not to dissect lateral and inferior to Cooper's ligament, as the Iliac Artery and Vein will enter the femoral canal at this site.

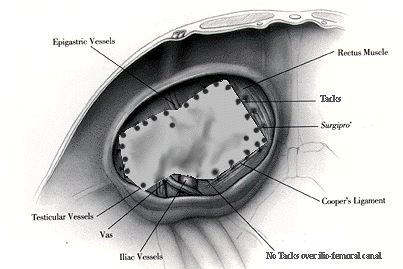
STEP 4: Inserting and Anchoring the Mesh
The graft of SurgiPro* Mesh (Open Weave) is inserted uncut into the intra-abdominal cavity and deployed over the inguinal region. The graft is attached or secured to Cooper's Ligament, around and lateral to the Inferior Epigastric Vessels using tacks delivered via the Protack* Instrument. This instrument is dramatically different from the classical Multifire EndoHernia* stapler. The tacks are inserted by rotating; these tacks are more secure than the endostaples, and in most cases, we use 25 to 30 tacks (one disposable instrument) to perform one repair. Again, the operator should be meticulous to avoid the iliac vessels.
It should be noted, this instrument does not bend, but tacks can be safely placed or inserted at all angles. It differs from the use of the Multifire EndoHernia* stapler; abdominal wall counter pressure can be used here.
STEP 5: Closing the Peritoneum
Finally, the peritoneum is closed using the same tacks. With these repairs, we have a tendency to develop a larger inferior peritoneal flap in order to overlap both peritoneal incisions to tack them closed. The trocars are removed upon completion of this repair, and the 5 mm trocar sites are, of course, not closed on a facial level.