|
|
INTRODUCTION |
|
During the last
For many procedures, such as removal of ectopic pregnancies and treatment of endometriosis, the
cost-to-benefit ratio is well established, particularly in terms of expense and
safety. For other procedures, including laparoscopically
assisted hysterectomy and staging of gynecologic cancers, the ultimate utility
of this approach remains to be clearly defined.
History of the Procedure: Laparoscopy was first performed
in animals in the early
Problem: Laparoscopy is a unique surgical approach that
shares characteristics of both minor and major surgery. To patients,
laparoscopic procedures often are considered to be minor surgery because of
small incisions, a relatively small amount of postoperative pain, and short
convalescent period. If a laparoscopic procedure involves
minimal intra-abdominal surgery (eg, diagnostic
laparoscopy, tubal fulguration), both postoperative
discomfort and risk of complications may more closely resemble a minor
procedure than a major procedure.
At its essence, laparoscopy remains an intra-abdominal
procedure. It therefore shares all intraoperative and
postoperative risks of laparotomy, including
infection and injury to adjacent intra-abdominal structures. When major
intra-abdominal procedures are performed laparoscopically
(eg, hysterectomy), the resultant postoperative pain
and morbidity are still significant, but they always are less significant than
similar major surgery performed by laparotomy since a
large abdominal incision is unnecessary.
Laparoscopic procedures have unique risks, which are
related to methods used for placement of abdominal wall ports and to the pneumoperitoneum required for laparoscopy. These risks
include injury to bowel, bladder, or major blood vessels, and intravascular insufflation. In addition, increased intra-abdominal
pressures associated with laparoscopy increase anesthesia-related risks such as
aspiration and increased difficulty ventilating the patient. Although risk of
blood loss is relatively low for most procedures, potentially massive blood
loss may occur and is complicated by the fact that control of blood loss may be
delayed by the time taken to perform an emergency laparotomy.
Frequency: Laparoscopy is one of the most common surgical
procedures performed in the
|
|
INDICATIONS |
|
Diagnostic laparoscopy
Frequently, the physician needs to assess the pelvis for
acute or chronic pain, ectopic pregnancy,
endometriosis, adnexal torsion, or other pelvic
pathology. Determination of tubal patency
also may be an issue. Usually, the camera lens is placed infraumbilically
and a second port is placed suprapubically to probe
systematically and observe pelvic organs. If needed, a biopsy can be obtained
to diagnose endometriosis or a malignancy. If tubal patency is a concern, use of a uterine manipulator with a cannula allows a dilute dye to be injected transcervically (chromopertubation).
Tubal sterilization
Trocar placement is similar
to diagnostic laparoscopy. Bipolar electrosurgery,
clips, or silastic bands may be used to occlude the
tubes at the mid-isthmic portion, approximately
Lysis of adhesion
Adhesions may form due to prior infection, such as a
ruptured appendix or pelvic inflammatory disease (PID), endometriosis, or
previous surgery. Adhesions may contribute to infertility or chronic pelvic
pain. Adhesions may be lysed by blunt or sharp
dissection. Aquadissection may aid in the development
of planes prior to lysing. Any of the power instruments
may be utilized for cutting and coagulation. Unipolar
electrosurgery, such as the fine unipolar
needle, should be limited to adhesions
Adhesions may reform after lysis,
although this can be reduced with good hemostasis.
Surgeons frequently utilize intraperitoneal
anti-inflammatory solutions of steroids and dextran-
Fulguration of endometriosis
Endometriotic lesions may be resected or ablated using any of the power
instruments. This has been shown to improve fertility and decrease pelvic
pain.
Treatment of ectopic pregnancy
Laparoscopy is the surgery of choice for most ectopic pregnancies. A salpingostomy
or salpingectomy may be used to remove the embryo and
gestational sac. Auxiliary instruments, such as pre-tied loops or stapling
devices, may be particularly well suited for the salpingectomy,
although any of the power
instruments work equally well.
Ovarian cystectomy
If an ovarian simple cyst sized
The cyst can be removed by a number of techniques. If the
cyst is complex, rule out malignancy by looking for signs of ascites, excrescences on the ovary, or implantations on the
peritoneal, liver, or diaphragmatic surfaces. If malignancy is not apparent,
carefully dissect the cyst, making an effort to remove the cyst intact. A bag
may be used to transfer the cyst out of the peritoneal cavity through a
If the cyst ruptures during removal, liberally rinse the
peritoneal cavity with lactated Ringer's solution. A dermoid
cyst is particularly concerning due to contamination of the peritoneal cavity
with sebaceous material, causing a chemical peritonitis. Fear of seeding the cavity
with a malignant tumor always has been present, although recent data suggest
that spilling does not alter prognosis if a staging laparotomy
is carried out immediately. Postmenopausal cysts also may be removed by
laparoscopy, although with the increased concern for malignancy, an oophorectomy and laparotomy may
be more prudent. Physicians who perform a laparoscopy should be comfortable
with staging by laparoscopy or laparotomy, and
malignancy should be ruled out perioperatively.
Oophorectomy
As stated above, an oophorectomy
may be more appropriate in postmenopausal women with a growing or persistent
cyst. A tubal pregnancy or large hydrosalpinx
with adhesions also may require ovary removal. The power instruments, pre-tied
loops, or stapling devices may be used to occlude the infundibular
ligament and safely remove the ovary. Because of ovary size, a retrieval bag is
needed to remove the tissue. Options for removing the ovary from the peritoneal
cavity include using a
Myomectomy
Many women with a symptomatic fibroid uterus prefer myomectomy to hysterectomy in order to preserve fertility
or the uterus. If the patient has a pedunculated
fibroid, the stalk may be easily incised. For intramural fibroids, however,
risk of bleeding increases. An injection of vasopressin into the uterus may
help maintain hemostasis. The defect left by the
fibroid must be sutured, which can be difficult by laparoscopy for the
inexperienced. Barrier techniques may be used to decrease adhesion formation.
The fibroid may be removed by morcellation
or colpotomy. Power morcellators
are available to expedite the process. To date, laparoscopy has not proven
better than laparotomy for treatment of menorrhagia or infertility. In addition, some concern
exists that the risk of subsequent uterine rupture during pregnancy may be
greater after myomectomy performed by laparoscopy than
by laparotomy.
Hysterectomy
Initially, laparoscopy was performed prior to vaginal
hysterectomy to restore normal anatomy. Currently, however, it often is used in
a variety of ways, such as assessing feasibility of a vaginal hysterectomy
(when suspecting adhesions, endometriosis, or large fibroid uterus) and
performing some or all of the actual hysterectomy. The
LAVH is the most commonly employed and technically straightforward
of the
LH, the second approach, is performed initially like the
LAVH, except that the entire hysterectomy is performed laparoscopically.
The surgeon would choose indications similar to LAVH but would add lack of
uterine descent, which would make the vaginal approach impossible. After the infundibular, utero-ovarian, and
round ligament are occluded and divided, the bladder is dissected off the
uterus anteriorly. The ureter
is identified and dissected along its entire course, and then the uterine
vessels and uterosacral ligaments are occluded and
divided. After the posterior cul-de-sac is incised, the specimen is removed
vaginally and the cuff is closed.
LSH is the third approach, being most often promoted for
benign indications. The technique begins again as for the LAVH, but proceeds
with separating the entire fundus from the cervix
after the proximal vessels are divided and the bladder is dissected away from
the uterus. A special instrument is used to core out or cauterize the endocervix, and then the uterus is removed through a
Oncologic procedures
Laparoscopy originally was used in oncology for
second-look procedures following surgical and chemical treatment of malignancy.
With time, staging, including peritoneal washes with biopsy, partial omentectomy, and pelvic and periaortic
lymphadenectomy, was done laparoscopically.
Some oncologists believe the laparotomy can then be
avoided. Procedures such as laparoscopically assisted
radical vaginal hysterectomy also have been developed.
The laparoscopic approach in gynecologic oncology remains
very controversial and must be done with the same care (inspecting the entire
peritoneal cavity and pelvic structures) as with laparotomy.
Until the risk, benefits, and effects on long-term prognosis have been shown to
be equal to laparotomy, the laparoscopic approach
will remain under close scrutiny.
|
|
RELEVANT
ANATOMY AND CONTRAINDICATIONS |
|
Relevant Anatomy: Anterior abdominal wall anatomy
should receive special attention prior to laparoscopy since many laparoscopic
complications result from trocar placement.
Abdominal scars
As noted above, previous surgery
is associated with a greater than
In addition to location, the width and depth of the scar
should be evaluated, since a wide or retracted scar may suggest that a
postoperative wound infection had occurred. It is common wisdom that
postoperative infections may be associated with an increased risk of
intra-abdominal adhesion formation, although no data are available to support
this observation. If the dome of the bladder is involved in the infectious
process, it may cause progression of the bladder dome higher behind the
anterior abdominal wall, thus increasing the risk of bladder injury at the time
of suprapubic trocar
placement.
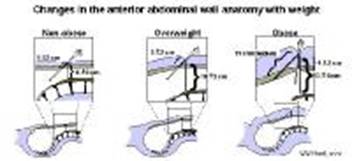
Abdominal wall thickness
Although abdominal thickness correlates with patient
weight, short stature or truncal obesity may increase
abdominal wall thickness out of proportion to patient weight. Routine
evaluation of the abdominal wall prior to laparoscopy is important since the
success of trocar insertion may depend on altering
the technique based on abdominal wall thickness.
Umbilicus
The umbilicus should be examined for signs of umbilical
hernia. Techniques for trocar insertion should be
adjusted, and closure of the defect should be considered. In the absence of
incarcerated bowel, the skin over the hernia can be carefully incised and the
peritoneal cavity entered using an open technique. Closure of a small defect
can be performed with interrupted sutures at the completion of the laparoscopic
procedure. Larger defects may require the assistance of a surgeon experienced
in umbilical hernia repair for ideal cosmetic results.
Contraindications: Determination of absolute
contraindications to laparoscopy remains controversial. For years, previous
abdominal surgery and intestinal obstruction were regarded as contraindications
to laparoscopy because of an increased risk of iatrogenic bowel perforation.
Recent reports, however, suggest that morbidity is lower with the laparoscopic
approach than with laparotomy. In gynecology, the
most commonly suggested contraindication is hemodynamic
instability resulting from an unruptured ectopic pregnancy. Following appropriate fluid
resuscitation, however, laparoscopy is a safe approach. Another traditional
contraindication was pregnancy. In the last few years, several large series
have documented the safety of laparoscopy during pregnancy with the use of an
open technique. Finally, disagreement is ongoing as to whether a known
gynecologic malignancy is a contraindication to laparoscopy. Several case reports
and series have suggested that laparoscopy may increase the risk of intraperitoneal spread of cancer cells.
Although few absolute contraindications exist for laparoscopy, several risk
factors are well appreciated.
Patient risk
factors
Obesity
It is well appreciated that obesity increases the risk of
any abdominal surgery. For laparoscopy, increased weight takes on a special
significance. Women with a body mass index (BMI) greater than
In women who are overweight, and even more so in those
who are obese, every aspect of laparoscopy becomes more difficult and
potentially more risky. Placement of laparoscopic instruments becomes much more
difficult and often requires special techniques. Bleeding from abdominal wall
vessels may become more common since these vessels become difficult to locate.
Many intra-abdominal procedures become increasingly difficult because of a
restricted operative field secondary to retroperitoneal fat deposits in the
pelvic sidewalls and increased bowel excursion into the operative field. This
second problem probably is related to increased volume of bowel, decreased
elevation of a heavier anterior abdominal wall by the pneumoperitoneum,
and the inability to place many obese patients in steep Trendelenburg
because of ventilation considerations.
Weight loss prior to elective surgery in overweight and
obese patients would be ideal. Unfortunately, significant weight loss may take
years and, more often than not, is impossible. A more realistic approach is to
inform the patient of the increased risk associated with obesity, and limit the
extent of advanced laparoscopic procedures that are attempted in obese
patients. Although no certain weight exists at which laparoscopy is
contraindicated, many surgeons hesitate to perform all but the simplest
laparoscopic procedures in patients weighing over
Age
Another well described surgical risk factor is age. As
the population ages, more women of increased age will have indications for
laparoscopy. Older patients are at increased risk of having concomitant disease
processes that affect their perioperative morbidity
and mortality.
Probably the single most important consideration is
age-associated increase in cardiovascular disease. Risk is increased even
greater in women who have not taken replacement hormones after menopause. Intraoperative cardiac stress related to anesthesia and the
surgery itself may result in sudden cardiac decompensation
based on arrhythmia, ischemia, or infarct.
Of special importance is the increased susceptibility of
the elderly to hypothermia since the vast majority of patients experience some
degree of hypothermia during laparoscopy. In older patients, even mild degrees
of hypothermia may increase the risk of cardiac arrhythmia and prolong recovery
time.
Previous abdominal surgery
As far as laparoscopic complications are concerned, one
of the most important risk factors is a history of previous abdominal surgery.
The risk of adhesions of omentum and/or bowel to the
anterior abdominal wall after previous abdominal surgery is greater than
The most common of these strategies is the use of an open
technique for laparoscopic trocar placement, as first
advocated by Hasson. Open laparoscopy techniques
almost certainly decrease the risk of bowel injury distant to the umbilicus. To
avoid bowel injury at the site of entry, modifications of the open technique
have utilized blunt entry of the peritoneal cavity with a hemostat to avoid
inadvertently grasping and incising the bowel. In patients with previous laparotomy in which the scar is located at the umbilicus,
use of an alternative location (usually in the left upper quadrant) has been
recommended for trocar insertion to avoid injury of
bowel adherent immediately beneath the umbilicus. Since not much is known about
the rate of injuring structures in this area (eg,
spleen, colon, common iliac vessels), when using a closed insertion technique,
it may be prudent to use an open approach in this alternative location for trocar insertion.
Despite the potential for increased risk of bowel injury
after previous laparotomy, some laparoscopists
advocate the use of a closed periumbilical trocar insertion techniques in all patients, regardless of
a history of previous surgery. One justification is that bowel injury is
uncommon (approximately
Anesthetic risk
factors
Anesthesiologists are trained not only in the art of
providing anesthesia, but also to serve as consultants. This may be one of the
least utilized assets available to modern surgeons. Prior to surgery, discuss
preparation of any patient with significant health problems with an
anesthesiologist. In complex cases, these patients should be seen by an
anesthesiologist for optimal preanesthesia
preparation.
Time since last oral intake
One of the most critical time-dependent aspects of
preparation is the degree to which the patient's stomach is empty, since both
general anesthesia and increased intra-abdominal pressure may increase risk of
regurgitation and resultant aspiration. The appropriate time to wait from the
last oral intake until induction of general anesthesia is a much-debated topic.
In general, it is recommended that approximately
Unfortunately, in emergency cases such as ectopic pregnancy or ovarian torsion, general anesthesia
may be required despite a period of fasting of less than
Heart disease
Preoperative evaluation should search for evidence of
underlying cardiac disease. With a positive history or physical findings
suggestive of cardiac disease, preoperative evaluation by both a cardiologist
and an anesthesiologist is extremely important. Patients with ischemic heart
disease who undergo anesthesia may have decreased cardiac blood return coupled
with an increase heart rate that may result in infarction.
Laparoscopic-associated metabolic acidosis, respiratory acidosis, and
hypothermia may result in arrhythmia in predisposed patients, thus increasing
the risk of ischemia even further. There also is an increase of arrhythmia with
distention of the abdomen, especially in patients who are spontaneously
breathing.
Finally, patients at risk for congestive heart failure
should be evaluated carefully prior to laparoscopy since a decrease in cardiac
output may be related to decreased venous return and
increased peripheral vascular resistance.
Pulmonary disease
Any patient with significant history of pulmonary
problems should be evaluated by both a pulmonologist
and an anesthesiologist prior to laparoscopy. When given an option, laparoscopy
is preferable to laparotomy in these patients. The
relatively decreased postoperative pain following laparoscopy may result in
less ventilatory compromise than laparotomy
and thus fewer problems with atelectasis or pulmonary
failure in those with borderline pulmonary function.
Special care should be taken with patients with pulmonary
disease during laparoscopy. Hypercarbia and decreased
ventilation associated with laparoscopy may be especially deleterious in
pulmonary patients with chronic respiratory acidosis. In rare cases, pneumothorax and pneumomediastinum
have been described as complications of abdominal insufflation.
In patients with compromised pulmonary function, even a small intravasation of carbon dioxide could result in significant
pulmonary decompensation.
|
|
WORKUP |
|
Lab Studies:
- Complete blood
count
- In general, one
of the few required laboratory evaluations in a healthy patient is a
complete blood count (CBC).
- Anemia
increases the risk of anesthetic complications and infections, both at
the operative site and the skin incision. In addition, an anemic patient
has less of a safety margin in the uncommon case of significant operative
blood loss. For elective surgery, every effort should be made to provide
effectual treatment for anemia prior to surgery.
- Pregnancy Test
- Many surgeons
recommend routine pregnancy tests for all patients prior to elective
surgery, since both surgery and anesthesia should be avoided during
pregnancy. Although the most commonly used anesthetics show little
evidence of either teratogenicity or increased
risk of spontaneous abortion, the medicolegal
implications of electively performing surgery and administering
anesthesia during pregnancy justifies establishing pregnancy status prior
to surgery. Exceptions are usually made for patients who were surgically
sterile or who are known to be pregnant.
- A urine
pregnancy test is adequate in most cases, since these modern tests
accurately detect beta-hCG levels of
- An alternative
to performing routine pregnancy tests prior to surgery is to schedule all
elective surgery during the follicular phase (i.e., within
- Urinalysis
- Many laparoscopists obtain a urinalysis prior to surgery.
Urinalysis may detect an unsuspected systemic disease, such as diabetes,
which should be completely evaluated prior to elective surgery.
- More commonly, urinalysis may indicate the presence of a subclinical urinary tract infection that may be
exacerbated by catheterizing the patient. Treating these infections prior
to surgery may avoid postoperative discomfort and potentially serious sequelae in susceptible patients.
- Other laboratory
evaluations
- In patients with known health problems, other laboratory tests, such
as liver function tests or electrolytes, may be indicated.
- A thorough
preoperative medical evaluation, including appropriate laboratory
studies, is appropriate in anyone with significant medical problems.
Imaging Studies:
- Chest
radiography
- A routine preoperative chest radiograph (CXR) probably is
unnecessary for patients with no risk factors.
- In patients
with coexisting bronchopulmonary conditions,
cardiac conditions, or abnormal clinical cardiopulmonary findings, a
preoperative CXR certainly is important. CXR also is part of the basic
workup for anyone suspected of having a gynecologic malignancy.
- Intravenous pyelograph or kidney ultrasound
- Radiographic or sonographic evaluation of
the urinary tract is important in women with uterine anomalies, those
known to have severe endometriosis, and those with an ovarian mass fixed
in the pelvis. Women with uterine anomalies are at risk for concomitant
urologic anomalies; thus, an intravenous pyelogram
should be performed to determine kidney location and the state of the ureters.
- In select cases of severe endometriosis or when a fixed pelvic mass
is present, preoperative evaluation for possible ureteral
involvement also is important. Hydronephrosis,
indicating partial or complete obstruction of the ureter,
can be ruled out using kidney ultrasound in these cases.
- Barium enema
- Severe endometriosis can sometimes involve the colon. In patients
with colonic symptoms, such as cyclic hematochezia,
or narrowing caliber of stool, a preoperative barium enema with air
contrast is important.
- Alternatively, colonoscopy may be helpful in patients with these
suggestive symptoms.
Other Tests:
- Electrocardiogram
- A routine preoperative electrocardiogram (ECG) prior to laparoscopy
is not indicated in a young, healthy woman. A preoperative ECG should be
considered in all women over the age of
- In addition, any woman with a history of cardiac disease or any
physical finding or disease history that puts her at increased risk of
cardiac disease (eg, diabetes mellitus,
hypertension, thromboembolic diseases, stroke,
renal impairment, chronic pulmonary disease) should have a preoperative
ECG regardless of age.
|
|
TREATMENT |
|
Surgical therapy:
General
techniques for laparoscopy
Primary trocar placement
Numerous techniques exist for creating a pneumoperitoneum and placing a laparoscopic port into the
abdomen. Each is purported to offer a unique advantage. Four common approaches
are Veress needle insertion followed by a primary trocar insertion, direct trocar
insertion, open laparoscopy, and optical trocar
placement. Physician experience significantly contributes to the safety of the
individual technique. Both reusable and disposable instruments are available.
Choice of instrumentation should take into account the condition of the
available reusable equipment and cost of the disposable equipment.
Veress needle and primary trocar insertion
When the Veress needle is
placed through the umbilicus into the peritoneal cavity, avoidance of both the
retroperitoneal vessels and the intestinal tract is of paramount importance.
The patient must be in the complete horizontal position (not Trendelenburg) and the patient's body habitus
should be carefully assessed (Picture 1).
The abdominal wall is elevated by manually grasping the skin and subcutaneous
tissue to maximize the distance between the umbilicus and the retroperitoneal
vessels. An alternative method for elevation is to place penetrating towel
clips at the base of the umbilicus.
In the average-weight person, the lower anterior
abdominal wall is grasped and elevated, and the Veress
needle is inserted toward the hollow of the sacrum at a
Correct placement of the Veress
needle may be confirmed by a number of methods, such as the hanging drop test,
injection and aspiration of fluid through the Veress
needle, or measurement of intra-abdominal pressure with carbon dioxide insufflation. After a pneumoperitoneum
has been achieved with a Veress needle, the primary trocar with sleeve (most commonly
Direct trocar insertion
Direct trocar insertion refers
to inserting the primary trocar without having
previously inserted the Veress needle and
insufflating the abdomen with carbon dioxide. The primary trocar
is inserted in a manner similar to Veress needle
insertion. The sleeve from the trocar is then used to
insufflate the abdomen with carbon dioxide. Although several small studies
suggest that the safety of this technique is equal to Veress
needle, subsequent larger studies report a bowel injury rate of
Open laparoscopy
Open laparoscopy involves incising the anterior rectus fascia and bluntly entering the peritoneal cavity
with a Kelly or Crile clamp. A blunt-tipped trocar with sleeve is then placed into the peritoneal
cavity. For the Hasson technique, sutures used on the
fascia hold the sleeve in place and anchor the sleeve to help maintain a pneumoperitoneum. Because this method almost completely
avoids the risk of retroperitoneal vessel injury and may decrease the risk of
bowel injury, some laparoscopists use this approach
exclusively. Many laparoscopists use this method for
patients with risk of abdominal adhesions.
Expanding Access Cannulas
A relatively new technique for laparoscopic trocar placement is the use of expanding access cannulas. This technique involves the placement of a Verres needle for insufflation.
After the peritoneal cavity is insufflated, the Verres
needle is removes and reinserted after it is place into an expandable sleeve.
Once the needle and sleeve are placed into the peritoneal cavity, the needle is
removed and the sleeve dilated up to a
Optical trocar technique
A clear trocar has been
developed to penetrate the abdominal layers while visualizing the layers with
the laparoscope inserted in the trocar (Endopath Optiview trocar, Ethicon Endo-Surgery,
Inc,
Placement of secondary trocars
Secondary trocars are required to perform most gynecologic
laparoscopy procedures, with the exception of some diagnostic laparoscopies.
After identifying the epigastric vessels by transillumination and intraperitoneal
observation,
The trocars are placed either in the midline,
Expanding Access Cannulas for Secondary Trocar Placement
The relatively new
expanding access cannula technique described above
was initially developed for placement of secondary laparoscopic trocars. This technique involves the placement of a Verres needle in an expandable sleeve through the abdominal
wall at the desired site under direct visualization. Once the needle and sleeve
are placed, the needle is removed and the sleeve dilated up to a
Power instruments
Monopolar electrosurgery was the first
methodology used for laparoscopic coagulation. In the past
Techniques for large
vessel occlusion
As laparoscopy has
become more prominent in gynecology, techniques have been designed to offer
efficient means of tying and cutting large vessels, such as ovarian and uterine
vessels. Traditional suturing with intracorporal or extracorporal knot-tying has been used effectively, but for
most surgeons is relatively difficult and slow. The first technique developed
to assist in occluding large vessels was the pre-tied suture loop (Endoloop, Ethicon Endo-Surgery,
Inc,
More recently, new
instruments have become available to aid in the suturing process. In addition,
linear stapling devices have been used for occluding vessels during removal of adnexal structures or laparoscopic hysterectomy (Endo GIA
II stapler, United States Surgical Corporation, Auto Suture Company Division,
Preoperative details:
Preoperative medications
Estrogen replacement
therapy
In postmenopausal
women, estrogen replacement therapy (ERT) is an excellent preoperative adjuvant
from several perspectives. If surgery for pelvic relaxation (such as vaginal
vault suspension) or for urinary incontinence (such as laparoscopic Burch
procedure) is planned, several months of ERT prior to therapy will
significantly increase tissue thickness, resilience, and blood supply. Well estrogenized genitourinary tissue will make the necessary
repair much simpler and may reduce risk of operative site infection.
On a more general
level, women using ERT are known to have a lower risk of coronary heart
disease; therefore, they also may be reasonably expected to have a decreased
risk of cardiovascular complications during surgery.
Gonadotropin-releasing hormone
agonists
On the opposite end
of the spectrum are premenopausal women who may
benefit from temporarily decreasing levels of circulating estrogen by the use
of a gonadotropin-releasing hormone (GnRH) agonist. The most common situation in which this is
helpful is in the presence of large leiomyoma when
size alone makes surgery difficult. This is most common when hysteroscopic resection of a large submucosal
leiomyoma is to be attempted or when laparoscopically assisted vaginal hysterectomy is planned
for a markedly enlarged uterus. In general, uterine volume can be decreased by
up to
Prophylactic antibiotics
Prophylactic
antibiotics are a well established method of decreasing risk of postoperative
infections after either vaginal or abdominal hysterectomy. Although their use
has not been studied in a large number of cases of laparoscopically
assisted hysterectomy, it makes intuitive sense that prophylactic antibiotics
would be beneficial in these patients as well.
Another group of
patients who may benefit from prophylactic antibiotics are women undergoing tubal reconstructive surgery for pelvic adhesive disease
resulting from previous pelvic infections. Since these patients appear to be at
increased risk for postoperative infections after genital surgery, use of an intraoperative broad-spectrum antibiotic given
intravenously seems reasonable.
Oral contraceptives
Risk of postoperative
thromboembolism appears to be increased by the
preoperative use of high-dose oral contraceptives (
Although some authors
believe that oral contraceptives should be discontinued
Preoperative gastrointestinal preparation
Bowel preparation
If significant enterolysis is planned and either endometriosis or pelvic
adhesions are known or suspected to be present, preoperative bowel preparation
decreases risk of serious postoperative sequelae.
Although a multitude of bowel preparations have been described, the most common
oral agents used are either magnesium citrate or a polyethylene glycol
solution. Unfortunately, a thorough bowel preparation often is uncomfortable
for the patient. In high-risk patients, however, preoperative bowel preparation
may allow primary closure of an unplanned enterotomy;
in the presence of an unprepared colon, a temporary diverting colostomy may be
required.
Oral intake
"NPO after
Other preoperative considerations
Intravenous access
Because of the rare
but serious risk of sudden and potentially massive blood loss during
laparoscopy, establishment of intravenous access prior to starting the case is
required. Usually, this is in the form of a functioning intravenous catheter of
at least
Bladder
catheterization
Traditionally,
complete emptying of the urinary bladder with a catheter immediately prior to Veress cannula or trocar placement is performed to minimize the risk of
bladder injury. Some laparoscopists advocate having
the patient void immediately prior to entering the operating room. This
approach may, on occasion, be associated with the discovery of a significant
amount of bladder distention because of incomplete emptying or excellent urine
output. In-and-out catheterization appears to more consistently result in
compete bladder emptying and, when performed aseptically, appears to be associated
with minimal risk of iatrogenic urinary tract infection. For procedures of
longer duration, consider use of an indwelling catheter to avoid bladder
refilling, although this probably increases the risk of infection.
Deep vein thrombosis
prophylaxis
When
hysterectomy is planned, intraoperative and
postoperative use of pneumatic compression stocking with or without low-dose
heparin decreases risk of venous thromboembolic
complications. These measures also
should be considered in any patient whose ability to ambulate may be decreased
by conditions other than the planned surgery. After less extensive laparoscopic
procedures in healthy patients, risk of thromboembolism
appears to be small since most will be fully ambulatory
within hours of surgery. For these patients, methods for deep vein thrombosis
prophylaxis are not commonly used.
Patient positioning
Gynecologic
laparoscopy procedures usually are performed in the dorsal lithotomy
position to allow vaginal access for uterine manipulation. In the early days of
laparoscopy, this was attained by suspending the ankles in lithotomy
stirrups also known as candy cane stirrups. Unfortunately, these stirrups offer
little leg support, thus putting increased stress on both the knee and hip
joints. In addition, they require that patient be in high lithotomy
position, in which the thighs severely limit the range of movement of the
operator.
Most laparoscopists now use boot stirrups specially designed for
laparoscopy. These resemble obstetric stirrups in that they have a foot plate
and also support the popliteal fossa.
Laparoscopic stirrups, however, are more adjustable than those previously
designed for obstetrics. This avoids pressure on the lateral or posterior
aspect of the calf and permits easy positional changes from low lithotomy for laparoscopy to high lithotomy
for vaginal procedures, such as hysteroscopy or vaginal hysterectomy.
For low lithotomy, legs should be positioned so that the thigh is
slightly flexed, no more than
Once the primary trocar is placed, the patient is usually placed in no more
than
Skin preparation
Shaving of the pubic
hair above the symphysis may be required if hair
extends to the intended site of ancillary trocar
placement, usually
After changing
gloves, avoid contamination of both the abdominal field and instruments place
into the abdominal cavity. Prior to video laparoscopy, the operator's eye was
placed against the laparoscope, making it impossible to keep the operating
field sterile. Nevertheless, risk of infection involving the wound or the
peritoneal cavity after laparoscopy is extremely low, most likely because of
small incisions and decreased opportunity for intra-abdominal contamination.
With the advent of video laparoscopy, there is no reason that standard sterile
precautions cannot be applied to all laparoscopic procedures.
Intraoperative details:
Anesthesia considerations
Type of anesthesia
Over the years, many
methods of anesthesia have been employed for laparoscopy, including general
anesthesia, regional blocks, and local infiltration. Because of
Abdominal insufflation, usually with carbon dioxide at a pressure of
Increased
intra-abdominal pressure also is transmitted to the thorax. Pressure on the
diaphragm increases breathing effort in conscious patients. In patients under
general anesthesia, decreased excursion of the diaphragm can lead to atelectasis and functional pulmonary shunt, which in turn
can result in hypercarbia and a respiratory acidosis,
augmenting the acidosis associated with carbon dioxide absorption.
Abdominal insufflation can have direct cardiac effects as well.
Pressure on the intra-abdominal venous system can decrease the venous return to
the heart. Pressure transmitted to the right atrium decreases preload further.
This may be of minimal consequence in healthy patients, but it may lead to
cardiac compromise in those with borderline cardiac function.
Another aspect of
laparoscopy that can increase upper abdominal pressure is the use of Trendelenburg position to keep the bowel out of the pelvis.
The effects of gravity on intra-abdominal contents increases pressure on the
stomach and diaphragm, accentuating the problems discussed above.
Because of the
discomfort and risks associated with abdominal insufflation,
general anesthesia is the most common technique used for laparoscopy. To
minimize the risk of aspiration, endotracheal intubation also is recommended.
Local or regional
anesthesia should be used only in carefully selected patients. The chance of
significant discomfort and the risk of aspiration should be discussed
thoroughly with the patient, and only those able to handle some discomfort are
appropriate candidates. During laparoscopy, both the discomfort and the risk of
aspiration may be decreased by using the least intra-abdominal pressure
possible for insufflation (usually <
Postoperative
details: After any gynecologic laparoscopic
procedure, progressive resolution of symptoms during the first postoperative
Patients should be
counseled on the natural postoperative course of events and patients should be
instructed to contact their physician if any deviation from this course occurs.
A natural tendency may be to reassure a patient who calls that their
postoperative discomfort is within the normal range. This should be done with
caution, however, since delay of appropriate care often can compound the
effects of complications and may be fatal.
Probably the most
concerning postoperative symptom is worsening abdominal pain, especially in the
presence of distension. Signs of an occult injury of bowel or bladder may take
hours or days to develop. If a patient who calls the physician cannot be
assured with absolute certainty that she is not experiencing a surgical
complication, she should be advised to come in for an evaluation by someone
experienced in recognizing postoperative complications.
An unusual cause of
abdominal pain is an entrapped incisional hernia that
can occur after laparoscopy. Herniation is rare at
the site where the laparoscope is placed through the umbilicus. Bowel herniation, however, has been reported to occur when larger
trocars (>
Follow-up care: In the absence of complications, the patient should be
able to return to full activity within
Recovery from
laparoscopic hysterectomy can be expected within
|
|
COMPLICATIONS |
|
In addition to the traditional risks of surgery such as
infection and generalized bleeding, laparoscopy is a technique that presents
its own unique complications.
Gas embolism
Because carbon dioxide is used in laparoscopy to create
the pneumoperitoneum, a gas embolization
is an uncommon but very serious complication. Embolization
usually is caused by inadvertent placement of the Veress
needle in a major vessel prior to insufflation of the
abdominal cavity with carbon dioxide. Placement in the aorta or one of its
major branches allows carbon dioxide to escape into the vessel, which produces
temporary arterial occlusion. Usually the carbon dioxide is quickly absorbed
from the artery, and no serious results have been reported secondary to
arterial embolization. In these cases, arterial
bleeding would be the major complication. On the other hand, embolization of carbon dioxide into the venous system may
be fatal due to complete occlusion of the pulmonary artery by a large carbon
dioxide embolism.
To avoid this complication, the operator must verify intraperitoneal placement of the Veress
needle prior to insufflation. If one of the following
tests indicates malposition, the needle must be
repositioned:
- Open the Veress valve and observe for flow of blood from the abdomen
through the needle.
- Aspirate with a
syringe through the Veress needle.
- Administer the
hanging drop test by placing a drop of saline at the open end of the Veress, then observe if the drop disappears into the
shaft as the abdominal wall is elevated.
- Elevate the
abdomen with the Veress valve closed, then
assess for a hissing sound as the Veress valve
is opened. Alternatively, the Veress may be
attached to the insufflator with the valve in
the off position and the gas off. The abdomen is then elevated with the
valve open and a negative pressure reading will be observed on the insufflation instrument.
Recognition and treatment of a large venous embolization must be immediate. Clinical signs include
decreased end-tidal carbon dioxide, decreased oxygen saturation, a loud
mill-wheel murmur, severe hypotension, and possible cardiac arrest. Treatment
includes immediately stopping insufflation, removing
the needle, placing the patient in the left lateral decubitus
position, administering
Retroperitoneal major vessel injury
Laceration of major abdominal blood vessels is one of the
least common but most life-threatening complications in laparoscopy. Injuries,
which present in approximately
In theory, the aorta and inferior vena cava are avoided
if one inserts the Veress or trocar
through the umbilicus toward the hollow of the pelvis, since the umbilicus
usually lies over the bifurcation of the aorta at L
When placing the Veress needle,
the patient must be in the horizontal position (not Trendelenburg),
and the angle of entry varies depending on patient weight. Open laparoscopy
remains an alternative for avoiding retroperitoneal injury. Immediate
recognition of the injury is paramount to patient survival. If blood flows from
the open Veress needle or if the patient's vital
signs rapidly decompensate after Veress or trocar insertion, prompt action must be taken. With a
retroperitoneal hemorrhage, the peritoneal cavity may not show signs of
bleeding. If major vessel injury is suspected, notify the anesthesiologist in
order to place a central line and order blood products, make a midline incision
for good exposure, and immediately call a vascular surgeon. Although some
surgeons have advocated keeping the Veress needle in
place to mark the position of the injury, this approach has never been tested
and may actually impede definitive surgery or inadvertently enlarge the vessel
injury.
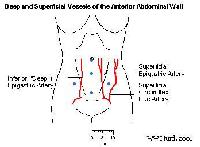
Abdominal wall vessel injury
As laparoscopy has become more sophisticated, the
placement of numerous and larger accessory trocars
lateral to the rectus muscles has increased the risk
of abdominal wall vessel injury. The primary vessels injured are the epigastrics (inferior and superficial) and the superficial
circumflex iliac (Picture 3).
The inferior epigastric originates from the external
iliac and the superficial from the femoral. Damage can lead to abrupt and
significant blood loss, producing a hematoma or
postoperative hemorrhage.
The first step to avoiding injury is
knowing the positions of these vessels. Often, the superficial vessels
can be seen by transilluminating the abdominal wall
with the laparoscope. The inferior epigastric artery
cannot be transilluminated but may be seen intraperitoneally beneath the peritoneum between the
insertion of the round ligament at the inguinal canal and the obliterated
umbilical artery. Prior to insertion of the lateral trocars,
the operator should make an effort to identify and avoid these vessels.
If unable to visualize the vessels, the operator can
enhance success for avoiding the vessels by placing the trocars
lateral to their usual location, which is
When an injury occurs, the operator must be prepared to
control the bleeding promptly. First, an attempt can be made to coagulate the
vessel with electrocautery. If another port is not
available to use electrocautery, a Foley catheter can
be placed through the trocar and the balloon inflated
with saline. Upward traction on the catheter, maintained with a clamp on the
abdominal side, will slow the bleeding until more definitive therapy can be
carried out. Once a second port is place, electrocautery
can be used. If this approach does not result in homeostasis, transabdominal sutures have been advocated. However, this
inexact approach has a risk of loosening in the immediate postoperative period.
A more secure technique is to enlarge the incision and selectively ligate the epigastric vessels,
which lie just below the rectus abdominus
muscle adjacent to the peritoneum.
Intestinal injury
Both the small and large intestine can be injured by
laparoscopy, posing a life-threatening situation for the patient if
unrecognized. If the patient has had previous abdominal surgeries or a history
of abdominal infections, such as PID or a ruptured appendix, risk of injury to
bowel adhered to the abdominal wall increases. Frequently, surgeons will choose
the open laparoscopy approach for these cases.
Recently, with the introduction of disposable trocars, the relative safety of these instruments has been
argued. The disposables have a safety shield, which is designed to extend over
the blade and decrease bowel injury with entry of the trocar
into the peritoneal cavity. These trocars are
extremely sharp and easily penetrate the fascia, which may cause additional
injury as the momentum of penetration continues into internal structures.
On the other hand, reusable trocars
may not be maintained regularly, and a dull trocar
pushed through the fascia with significant force may also abruptly pass through
the fascia and cause internal injury. No study has examined the relative safety
of disposable and reusable trocars, although one
series showed the risk of bowel injury with disposable trocars
to be approximately
Thermal injury to the bowel also is a risk when using electrocautery, particularly monopolar
cautery, which can cause an arc of electricity to the
bowel. This injury can cause peritonitis if unrecognized, and it is a
life-threatening situation if not promptly treated.
If injury is recognized at the time of surgery, immediate
action must be taken to repair the damage. Frequently, however, minor injuries
are not seen and manifest themselves
Urologic injuries
Injury to the bladder or ureters
can occur during trocar placement, use of power
instruments, or stapling or suturing devices. The greatest challenge is
recognizing that the injury has occurred so that the treatment can be performed
in a timely manner.
Draining the bladder with a catheter prior to trocar placement is the first step to preventing bladder
injuries. If urine is not seen in the pelvis but an injury is suspected,
intravenous indigo carmine can be given and the surgeon should watch for
leakage into the peritoneal cavity. If this is negative, but injury is still
suspected, a gravity cystogram may be performed.
Small retroperitoneal injuries may be treated with a Foley catheter for
Ureteral injuries can occur
with any procedure that uses instruments in the vicinity of the ureters. Thermal injuries from laser or cautery
may not be apparent for days after surgery. When a surgeon uses one of the
power instruments, the operator must be aware of the position of the ureter, and avoid cautery in
close proximity to the ureter. If the ureter is ligated, the patient
may present with flank pain secondary to hydronephrosis.
If the ureter is transected, the patient may develop a urinoma or ascites
and present
Incisional hernia
Before trocar and sleeves
larger than
|
|
FUTURE AND
CONTROVERSIES |
|
Laparoscopy continues to evolve as more sophisticated
instrumentation allows a greater variety of procedures to be performed. In the
past, many of these procedures would have been limited to laparotomy
and would have required a prolonged recovery period. The risks and benefits of
the procedures in many cases have not been fully evaluated. Some procedures,
such as tubal ligation, ectopic pregnancies, and simple lysis
of adhesions, appear to be safely and efficiently performed laparoscopically.
More complicated procedures, however, still need to be evaluated to determine
what is the safest and most efficient procedure.
The laparoscopic approach in gynecologic oncology remains
very controversial and must be done with the same care (inspecting the entire
peritoneal cavity and pelvic structures) as with laparotomy.
Until the risk, benefits, and effects on long-term prognosis have been shown to
be equal to laparotomy, the laparoscopic approach
will remain under close scrutiny.
|
|
PICTURES |
|
|
Caption:
Picture |
|
|
|
Picture Type: MRI |

|
Caption:
Picture |
|
|
|
Picture Type: Image |
|
Caption:
Picture |
|
|
|
|
|
|
|
|
Picture Type: Image |
|
|
|
BIBLIOGRAPHY |
|
- Azzam FJ, Padda GS, DeBoard JW: Preoperative pregnancy testing in
adolescents. Anesth Analg
- Bouillot JL, Fingerhut A, Paquet JC: Are routine preoperative chest
radiographs useful in general surgery? A prospective, multicentre
study in
- Chee SS, Godfrey CD, Hurteau
JA: Location of the transverse colon in relationship to the umbilicus:
implications for laparoscopic techniques. J Am Assoc Gynecol
Laparosc
- Clarke-Pearson
DL: Prevention of venous thromboembolism in
gynecologic surgery patients. Curr Opin Obstet Gynecol
- Fleites RA, Marshall JB, Eckhauser ML: The efficacy of polyethylene
glycol-electrolyte lavage solution versus
traditional mechanical bowel preparation for elective colonic surgery: a
randomized, prospective, blinded clinical trial. Surgery
- Godfrey C, Wahle GR, Schilder
JM: Occult bladder injury during laparoscopy: report of two cases. J Laparoendosc Adv Surg Tech A
- Harris MN, Plantevin OM, Crowther A:
Cardiac arrhythmias during anaesthesia for
laparoscopy. Br J Anaesth
- Hasson HM, Rotman C, Rana N: Open laparoscopy:
- Hawe JA, Garry R: Laparoscopic hysterectomy. Semin Laparosc Surg
- Hirvonen EA, Poikolainen EO, Paakkonen ME: The adverse hemodynamic
effects of anesthesia, head-up tilt, and carbon dioxide pneumoperitoneum during laparoscopic cholecystectomy. Surg Endosc
- Hirvonen EA, Nuutinen LS, Kauko M: Hemodynamic changes
due to Trendelenburg positioning and pneumoperitoneum during laparoscopic hysterectomy. Acta Anaesthesiol Scand
- Huezo CM, DeStefano F, Rubin GL: Risk of wound and pelvic infection after
laparoscopic tubal sterilization: instrument
disinfection versus sterilization. Obstet Gynecol
- Hurd WW, Pearl ML, DeLancey
JO: Laparoscopic injury of abdominal wall blood vessels: a report of three
cases. Obstet Gynecol
- Hurd WW, Wang L,
- Hurd WW, Bude RO, DeLancey JO: The relationship of the umbilicus to the
aortic bifurcation: implications for laparoscopic technique. Obstet Gynecol
- Hurd WW, Bude RO, DeLancey JO: Abdominal wall characterization with
magnetic resonance imaging and computed tomography. The effect of obesity
on the laparoscopic approach. J Reprod Med
- Hurd WW, Ohl DA: Blunt trocar laparoscopy. Fertil Steril
- Hutchison GL:
Oral contraception and post-operative thromboembolism:
an epidemiological review. Scott Med J
- Jones DB, Callery MP,
- Kaali SG, Barad DH: Incidence
of bowel injury due to dense adhesions at the sight of direct trocar insertion. J Reprod
Med
- Kim AH, Adamson
GD: Surgical treatment options for endometriosis. Clin
Obstet Gynecol
- Marcovich R, Del Terzo MA, Wolf JS: Comparison of transperitoneal
laparoscopic access techniques: Optiview
visualizing trocar and Veress
needle. J Endourol
- McCausland VM, Fields GA, McCausland
AM: Tuboovarian abscesses after operative
hysteroscopy. J Reprod Med
- McCleane GJ, McCoy E: Routine pre-operative
electrocardiography. Br J Clin Pract
- Meeks GR, Harris
RL: Surgical approach to hysterectomy: abdominal, laparoscopy-assisted, or
vaginal. Clin Obstet Gynecol
- Mettler L, Semm K, Shive K: Endoscopic
management of adnexal masses. J Soc Laparoendosc Surg
- Mintz M: Risks and prophylaxis in laparoscopy: a survey
of
- Moore SS, Green
CR,
- Mullett CE, Viale JP,
- Quint EH,
- Schemmel M, Haefner HK, Selvaggi SM: Comparison of the ultrasonic scalpel to
CO
- Szigetvari I, Feinman M, Barad D: Association of previous abdominal surgery and
significant adhesions in laparoscopic sterilization patients. J Reprod Med
- Tulandi T, Saleh A: Surgical
management of ectopic pregnancy. Clin Obstet Gynecol
- Twersky RS, Singleton G: Preoperative pregnancy testing:
"justice and testing for all". Anesth Analg
- Vecchio R,
- Westhoff C, Davis A: Tubal sterilization: focus on the
- Woolcott R: The safety of laparoscopy performed by direct trocar insertion and carbon dioxide insufflation under vision. Aust
N Z J Obstet Gynaecol
- Yim SF, Yuen PM: Randomized double-masked comparison of
radially expanding access device and
conventional cutting tip trocar in laparoscopy. Obstet Gynecol
- Yuzpe AA: Pneumoperitoneum
needle and trocar injuries in laparoscopy. A
survey on possible contributing factors and prevention. J Reprod Med