| Performing a Safe Laparoscopy - II |
| THE TELESCOPES |
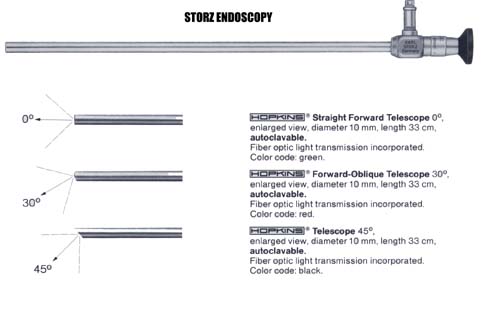
Telescopes or laparoscopes come in various sizes and with various visualization capabilities. For large telescopes, Storz Endoscopy has the best and widest choice of telescopes (from 13 mm to 2mm with Straight Forward 0 Deg. to 45 Deg.). We use four types of telescopes for all the interventional laparoscopic procedures we have described herein.
- Zero Degree Storz (Hopkins) Telescope: We exclusively use this telescope for Laparoscopic Repair of Inguino-Femoral Hernias. It is clearly inefficient in the performance of complex laparoscopic procedures.
- 30 Degree Storz (Hopkins) Telescope: This is the trocar we use preferentially for all advanced laparoscopic procedures.
- Zero Degree Storz (Hopkins) Telescope with 6 mm Instrument Channel: This telescope is used for single trocar laparoscopic appendectomy and Lap TAH-BSO.
- 2 mm United States Surgical Corporation 0 Deg. Telescope: This telescope is used for all Needleoscopic procedures.
We always have a 5 mm 30 Degree Telescope and a 10 mm Zero and 30 Degree Telescope available for ALL laparoscopic procedures..
We recently have been using 2 mm telescopes. These new MiniSite* 2 mm telescopes manufactured by the USS Corporation are part of the new generation of needleoscopic instruments. Initially, our surgical team felt these telescopes were of little value and the 2 mm instruments were too fragile. Newer 2 mm disposable and reusable instruments and telescopes were introduced. These have proven to be stronger and more durable therefore making this emerging field a definite feasibility (See chapter on Needleoscopic - 2mm procedures)
Most telescopes are reusable instruments. There are some multiuse-disposable telescopes which are as effective as the reusable. Some authors report the Surgiview* Zero Degree 10 mm laparoscope has been used as many as fifty times with the same effectiveness. This instrument could benefit smaller medical centers with a limited number of telescopes or as an additional laparoscope.
We have never used reusable trocars. The most dramatic technological advance in trocar design has been the VERSAPORT* trocar which we believe has become the best trocar on the market. The combination of a safety shield, consistent sharpness, immediate availability with no potential sterilization issues has made these trocars our first and exclusive choice. This is now the trocar type we use exclusively whenever available. In addition, this trocar has a reliable built in reducer mechanism allowing the surgeon to use instruments of different sizes. For example, a VERSAPORT* 12 to 5 mm can accommodate instruments ranging from 12 to 5 mm in size without any added reducer.
We only use standard disposable trocars and the following sizes:
A blunt trocar or so called Hasson Cannula should be available for use in the previously operated abdomen. We use the BluntPort* VersaPort* 5 to 12 mm.
For needleoscopic procedures, disposable 2mm MiniSite* Introducer trocars are used.
Unequivocally, the USSC ENDOCATCH* Specimen Pouch are the best specimen retrieval bags. They come in 2 sizes. A 10 mm small bag for gallbladder, appendix or small specimen and a 15 mm large bag used for large specimen retrieval such as the spleen.
Once the pneumoperitoneum has been created and sufficient intraabdominal pressure is maintained, the initial trocar can be inserted. Again the easiest site to insert this trocar is under the subumbilical area. An incision is made with a #11 scalpel. For a 10 mm trocar, a 8 mm incision is created to keep the skin snug around the trocar. The assistant or scrub nurse will exert direct pressure over the upper abdomen with their hand. This will raise the total intraabdominal pressure to a higher level while the trocar is inserted in the armed position toward the pelvis with gentle, rotating pressure.
Once this trocar is inserted, the other trocars can be inserted under direct vision.
Several techniques are used to place the first trocar in a patient who has undergone previous abdominal surgery. They are as follows:
1. The Open Insufflation Technique: A Blunt Trocar, or BluntPort* Trocar 5 to 12 mm, or Hasson Trocar is placed under direct vision by making a fascial incision, inserting the blunt trocar, securing it with sutures to the fascia and entering the intraabdominal cavity under direct vision. This is the safest technique in this clinical setting.
2. We routinely create a pneumoperitoneum with a Veress Needle as far away as possible from the old abdominal incision. A 5 mm trocar is then placed in the same position. Using a 30 degree 5 mm telescope, the intraabdominal cavity is visualized to place the additional trocars under direct vision.
Never attempt to place a trocar on the path of the epigastric arteries nor right under the costal margins (postoperative discomfort).
The surgeon needs to plan the placement of the trocar. Misplaced trocars will only impair the performance of this procedure.
Our guidelines for the fascial closure of trocar sites are simple and are as follows:
| Trocar Type | Fascial Closure |
| 2 mm MiniSite* Introducer | NO |
| 5 mm | NO |
| 10 mm (below the level of the Umbilicus) | YES |
| 10 mm (above the level of the Umbilicus) | NO |
| 12 mm | YES |
| 15 mm | YES |
| OBTAINING MAXIMUM VISUALIZATION DURING LAPAROSCOPY |
1. Immersing the telescope pre-operatively into warm saline for at least 15 minutes.
2. Do not use the trocar-telescope for insufflation. The insufflated CO2 will cool the telescope and prompt fog accumulation.
3. Use a defogging agent (FRED).
4. Intraabdominal wiping of the telescope: The tip of the telescope can be frequently wiped over intraabdominal organs for better visualization. It is best done on bowel surface. Omentum or fatty structures should be avoided.
5. Intraabdominal irrigation of the tip of the telescope: Some telescopes have built-in irrigation apparatus. The tip of the telescope can also be irrigated while working with a irrigation-suction device using normal saline. If the irrigated saline is cold this increased visualization will only be temporary.
To Go to Next Section