Laparoscopic
Appendectomy |
|
Although, the laparoscopic Appendectomy is not a new procedure, we believe it is about to become the Standard of Care Management for patients diagnosed with or suspected of having an acute appendicitis. The advent of high definition video-laparoscopy has developed laparoscopic appendectomy into an elegant, reliable procedure which can be easily performed. In most cases it can be completed within 20 to 30 minutes, and with experience, all clinical settings can be mastered. Critics of this procedure have claimed there are no significant cost savings and no improvement in the recovery of the patient. The following results will disprove these claims. It has been proven this procedure remains invaluable in patients with undiagnosed abdominal pain requiring further diagnostic intraabdominal exploration as well as patients with perforated appendicitis with or without an intraabdominal abscess.
This technique truly makes the appendectomy an outpatient procedure. The patient can resume a diet within a few hours after the "lap-appy" and in most cases can be discharged within 24 to 36 hours.
| THE STANDARD TECHNIQUE (ADULT PATIENTS) |
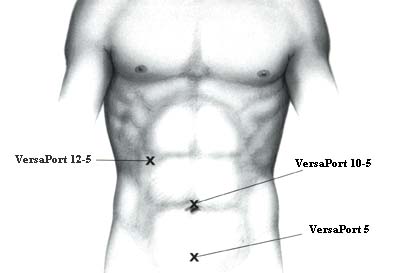
A pneumoperitoneum is obtained in the usual fashion. Three trocars are inserted: Two VERSAPORT* trocar 10-5mm (RUQ and Umbilical) and one 5 mm VERSAPORT* (Suprapubic). The operator should remember the telescope can be used alternatively between the RUQ and the Umbilical trocar. This can be quite useful in some clinical settings.
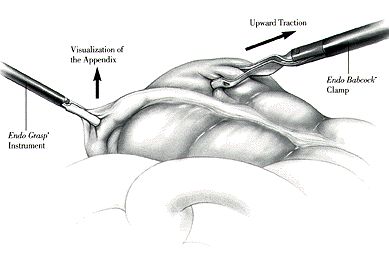
An atraumatic grasper or an ENDO BABCOCK*is inserted via the RUQ trocar. The cecum is retracted upward toward the liver. Im most cases, this maneuver will elevate the appendix in the optical field of the telescope. The appendix is grasped at its tip with a 5 mm claw grasper via the suprapubic trocar. It is held in upward position.
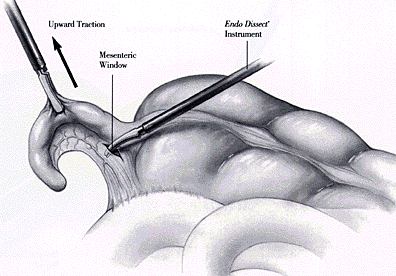
A dolphin nose grasper (or an ENDO DISSECT* instrument) is used to create a mesenteric window behind the base of the appendix. The window should be made as close as possible to the base of the appendix and it should be 1cm in size.
The appendix is transected by inserting an ENDO GIA* instrument via the RUQ trocar (blue cartridge, 3.5), closing it around the base of the appendix and firing it.
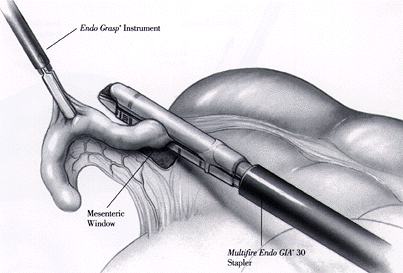
The base of the appendix is inspected for hemostasis. The operator should remember to wait five minutes before initiating measures to stop any bleeding site on the staple line as it will most likely stop within a few minutes. The ENDO GIA* cartridge is then changed to a vascular cartridge (white, 2.5) and the mesoappendix is stapled and transected with the same instrument. Several cartridges may have to be used.
The appendix is now amputated from the gastrointestinal tract. An ENDO CATCH*instrument is inserted via the RUQ trocar and deployed in the intraabdominal cavity. The appendix, held by the grasper (via the suprapubic trocar), is placed into the specimen bag. The bag is closed and the ENDO CATCH* instrument with the VERSAPORT* trocar is removed from the intraabdominal cavity. The ENDO CATCH*instrument is separated from the trocar, and the trocar is reinserted.
The intraabdominal cavity is irrigated thoroughly with normal saline (at least two liters). For perforated appendicitis with or without an intraabdominal abscess, a Blake Drain is left in the RLQ and pelvis.
| SINGLE TROCAR APPENDECTOMY (PEDIATRIC PATIENTS) |
| LAPAROSCOPIC APPENDECTOMY WITH SURGITIE* |
In this technique, three 5 mm trocars are inserted using the same locations as for the standard technique. A 5 mm 30 degree Storz telescope is used via the infraumbilical trocar. The dissection of the appendix is performed using atraumatic graspers as previously described. The mesoappendix is transected with ENDO SHEARS* instruments and ligated with an SURGITIE*. The tip of the appendix is then grasped after passing a second SURGITIE* around it. It is then ligated at its base and cut. The appendix is then removed via the infraumbilical site.
| NEEDLEOSCOPIC APPENDECTOMY |
This procedure can be done using newer, improved 2 mm MINISITE* instruments. Two 2 mm trocars are placed; one in the right upper quadrant and another one in suprapubic position. A VERSAPORT* 12 - 5 mm is placed in subumbilical position. using the same standard technique, this last port is used to insert the ENDO GIA* Stapler and to remove the appendix with an ENDO CATCH* Instrument.
![]()